Back
Symptoms of allergic rhinitis (or AR) vary from person to person and may alternate over time, even in the same individual. The term rhinitis refers to problems in the nose, but many people also experience symptoms that affect their eyes, mouth, throat, and ears.
Nasal symptoms:
Eyes:
Mouth – Throat:
Ears: The Eustachian tube connects the back of your nose to your middle ear (the air-filled space behind your eardrum). Allergic inflammation often affects this tube, especially in children. As a result, it can become harder to equalise the pressure in your ears, for example, when a plane descends. This may cause ear discomfort or a popping sensation. Children with allergic rhinitis (AR) are also more likely to develop glue ear (temporary hearing loss caused by fluid in the middle ear). Treating AR effectively can help reduce this problem.
Sinuses: the sinus linings can also swell with allergen exposure, leading to facial discomfort and making infection more likely. This happens because congestion reduces the normal drainage of mucus from the sinuses, allowing viruses or bacteria to become trapped, potentially leading to infection.
Chest: AR can make the lining of the lower airways more irritable, leading to symptoms such as coughing, wheezing, and shortness of breath. Effective treatment of AR helps prevent this and stops nerve signals that can trigger irritation in the lower airways. Allergic rhinitis also occurs in many people with asthma, where inflammation is already present in the lower airways. In this situation, both the upper and lower airways require treatment. Speak with your healthcare provider if you experience any chest symptoms.
Although people sometimes dismiss allergic rhinitis as a minor nuisance, it is a medical condition, and it can have a major impact on daily life.
Patients often describe their symptoms as bothersome, and they can disturb sleep, leaving people feeling tired during the day and making it harder to concentrate or think clearly. Many people find that their work or school performance suffers. Seasonal AR is associated with low grades in adolescents taking major examinations. Allergic rhinitis can have a major impact on overall quality of life if patients do not manage it well with medical treatment.
Moreover, when treatment is not properly done, allergic rhinitis can increase the risk of related conditions, including ear infections, sinus infections, and asthma. Poorly controlled allergic rhinitis may worsen asthma symptoms and increase exacerbations.
Healthcare professionals often classify allergic rhinitis based on how often symptoms occur and how much they affect daily life. This classification helps guide decisions about the most appropriate treatment.
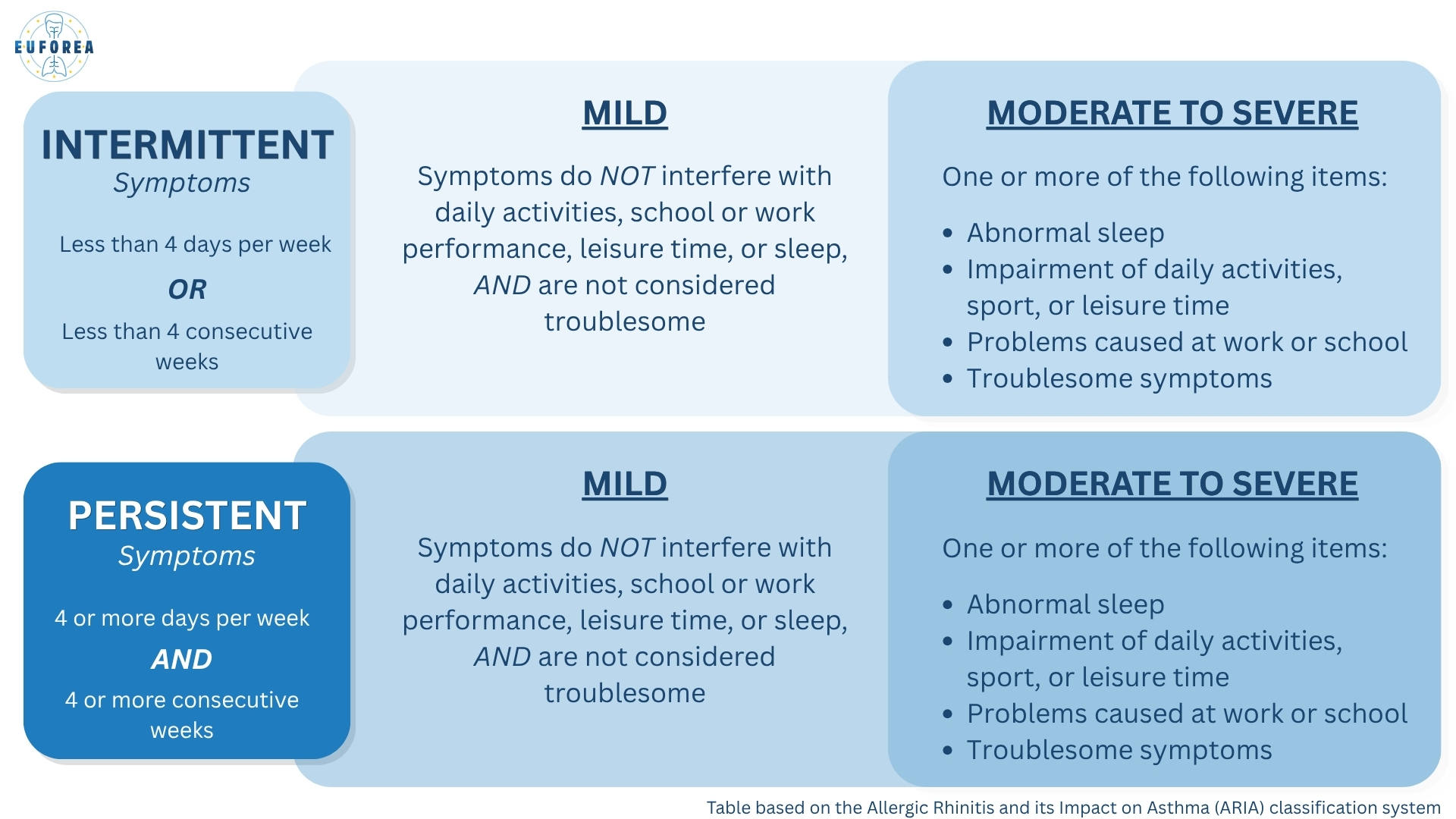
Although this classification system has its merits, it has also been criticised by the scientific community. For example, someone with symptoms 3 days a week all year round would technically be “intermittent”, even though their symptoms act more like persistent ones.
When allergen contact is intermittent, the initial nasal symptoms can be dramatic with sneezing, itching, and runny nose. When allergen exposure is persistent, the major symptom is often nasal blockage, with mucus dripping down the back of the throat (post-nasal drip), and the diagnosis can be sometimes be missed.
Allergic rhinitis is often self-managed with the support of a pharmacist, though you can always see your GP early on if you’d like a confirmed diagnosis and treatment guidance. The pharmacist can help determine whether your symptoms are likely caused by allergic rhinitis or another condition and guide you toward appropriate self-management options. Pharmacists are also trained to recognize when a referral to a GP is needed.
“Red-flag” symptoms that warrant a doctor’s visit:
NOSE:
EYES:
CHEST:
If none of the above-mentioned “red flag symptoms” are present, then you could self-treat, using the EUFOREA Patient Journey algorithm as a guide.
Step 1:
Important first steps are to avoid as far as possible those things that you find cause your symptoms. This could be an allergen or another non-specific trigger, like cigarette smoke. Find out more about these strategies in the Lifestyle and Prevention module.
Step 2:
Nasal saline rinsing helps keep your nose clean and reduces symptoms, making this a useful daily support in your allergic rhinitis self-management.
Step 3:
If these avoidance measures and rinsing with nasal saline are insufficient to control your symptoms, you could add a medicine from the list below. They are available over-the-counter in most countries.
Treatment options are:
- nasal corticosteroid sprays
- non-sedating antihistamine tablets
- nasal antihistamine sprays
In the self-management of allergic rhinitis: AVOID decongestants and sedating antihistamines.
Find out more information about each of these treatment options in our dedicated Treatment module.
All treatments for allergic rhinitis — including for people with intermittent symptoms — work best when taken consistently on a daily basis, starting before your symptoms usually do and continuing during the period they are needed. Avoid stopping and starting your medications, as irregular use makes them less effective.
If you’ve tried regular, daily treatment as above for your allergic rhinitis for at least two weeks but your symptoms are still bothering you, it’s a good idea to see your GP. They can check whether your symptoms are truly caused by allergic rhinitis or if something else might be going on. Allergy testing may be suggested, and your treatment plan will be optimized.
To get the most out of your appointment, you can look at our ‘Prepare for Your Consultation’ PDF. It helps you gather useful information ahead of time, such as an overview of your symptoms and a list of questions you may want to ask your doctor.
Your GP can prescribe a combination spray for you. This is a nasal spray that contains both a nasal corticosteroid and a nasal antihistamine. This is the most effective pharmacotherapy for people with AR. If this combination spray is not available/affordable where you live, you can use a nasal corticosteroid spray alongside a nasal antihistamine spray.
Alternatively, your GP may prescribe one of the other treatments mentioned below:
- leukotriene modifiers
- cromolyn nasal spray
- ipratropium bromide
- nasal or oral decongestants (only for short-term relief of severe nasal congestion)
If eye symptoms are the major problem or if they respond insufficiently to nasal treatment, then eye drops might be prescribed.
- antihistamine eye drops
- cromolyn/nedocromil eye drops
In some countries, you may need a GP referral before you can visit a specialist. Seeing an allergy specialist is important in the following situations:
Your specialist will adjust and improve your treatment plan and—in addition to the treatments you’ve already heard about above—can offer several extra options. These additional treatment options include:
- allergen immunotherapy
- short course of oral steroids
- surgery (for severe nasal obstruction)
Allergic conjunctivitis: This is an eye condition that happens when the conjunctiva (the thin, clear tissue that lines the inside of the eyelids and covers the white part of the eye) becomes inflamed due to an allergic reaction. It is not contagious, meaning you can’t pass it on to someone else.
Typical symptoms include intense itching, redness, and watery eyes. It is very common in people who have allergic rhinitis. In fact, around 7 out of 10 people with seasonal allergies also experience allergic conjunctivitis. People with perennial (year‑round) allergies can also develop these eye symptoms.
Food allergy: happens when the immune system wrongly recognizes certain foods as harmful, causing an allergic reaction. This reaction can affect the skin, stomach and gut, and respiratory system. Food allergies most often start in the first two years of life. Children with food allergies are more likely than their peers to develop allergic rhinitis and asthma later on. Even if the food allergy resolves, the increased risk remains.
Pollen-food allergy syndrome (PFAS, sometimes called oral allergy syndrome (OAS)), is a type of food allergy seen in people who have allergies to pollen. It happens because allergens in raw vegetables, fruit, and nuts are the same as or very similar to those in pollen (cross-reactivity). Common symptoms are itching of the mouth and throat. Severe reactions, such as anaphylaxis, are rare, but the gut can be affected. PFAS mostly affects people who have allergies to tree, grass, and weed pollen. It is estimated that between 5 and 7 out of 10 people with pollen allergies have PFAS. More information on PFAS, including a list of vegetables, fruits, and nuts to that might provoke symptoms can be found here.
Eczema, also referred to as atopic dermatitis, is a long-term inflammatory condition of the skin. It causes red, itchy, and inflamed skin that can be uncomfortable and persistent. People affected by eczema are more prone to developing other allergic conditions, such as asthma, allergic rhinitis, and food allergies. Studies show that up to 8 out of 10 children with atopic dermatitis may go on to develop allergic rhinitis and/or asthma later in life. Eczema most commonly develops during early childhood, before the age of 5, but older children and adults can develop the condition too.
Eczema is often an early step in the typical progression of allergic diseases from infancy into childhood. In the following video, a children’s allergist explains the concept of the allergic march, also often referred to as the atopic march.
A severe allergic reaction, called anaphylaxis, can occur with food allergies, drug allergies, and insect sting allergies. Anaphylaxis is a sudden, serious, and potentially life-threatening allergic reaction. It can develop very quickly—within seconds or minutes after exposure to an allergen—and requires urgent medical treatment.
If you have had a severe allergic reaction before, you will need to carry an adrenaline (epinephrine) auto-injector or nasal spray (availability depends on where you live) with you at all times. This allows you or someone nearby to give the injection as soon as the symptoms of anaphylaxis are recognised. Emergency services must always be contacted
Asthma: Having allergic rhinitis, whether seasonal or year-round, increases your chances of having asthma. In fact, up to 4 in 10 people with allergic rhinitis either have asthma or may develop it in the future, and some 60- 80 % of people with asthma have upper airway disease: rhinitis or rhinosinusitis. Asthma is a long-term condition that affects the lower airways (breathing tubes of your lungs). When you have asthma, the airways in your lungs become narrower and swollen, and can produce extra, sticky mucus. All of this makes it harder for air to flow in and out, so breathing becomes more difficult. If you recognize symptoms such as shortness of breath, chest tightness, wheezing, or coughing, see your doctor.
Chronic rhinosinusitis: People with allergic rhinitis have a higher chance of developing chronic rhinosinusitis. This is because allergies cause long-lasting inflammation (redness/swelling) inside the nose and sinuses. When these areas stay swollen over time, the small drainage pathways between the nose and sinuses become narrower. As a result, mucus can’t drain properly, which leads to nasal congestion, facial pressure, and an increased risk of ongoing sinus problems.
Sleep disturbances (including obstructive sleep apnea): A blocked nose is a common symptom of allergic rhinitis and can make it harder to breathe comfortably during sleep. This can lead to poor sleep quality, frequent waking, or trouble falling asleep.
Allergic rhinitis can also play a role in obstructive sleep apnea (OSA). Obstructive sleep apnea (OSA) is a condition where the upper airway briefly collapses during sleep, causing repeated pauses in breathing and therefore dips in the oxygen concentration in the blood. The frequent nocturnal dips in oxygen concentration can disrupt sleep and, over time, may affect overall health and quality of life.
Dental malocclusion (teeth misalignment): A blocked nose—a common symptom of allergic rhinitis—can cause someone to breathe through their mouth instead of their nose. Over time, mouth breathing can affect the normal growth of the face and jaws. In children, whose facial bones are still developing, this can increase the risk of dental misalignment (malocclusion) and changes in facial structure.
Ear problems (otitis media): Allergic rhinitis can sometimes lead to ear issues, especially in children. When allergies cause the inside of the nose to swell, this swelling can also affect the Eustachian tube (the small tube that connects the inner ear to the nose). If the Eustachian tube doesn’t work properly, fluid can build up behind the eardrum. This trapped fluid can then become infected by viruses or bacteria, leading to a middle ear infection (otitis media). This may cause ear pain, a feeling of fullness in the ear, and sometimes temporary hearing loss.
Impact on mental health: Allergic rhinitis is linked to a higher risk of anxiety and depression. Long-term nasal inflammation and sleep disruption from symptoms can impact your mental well-being. If your allergy symptoms are impacting your mood, energy, or daily functioning, talk to your healthcare provider. They can help treat your allergic rhinitis effectively and connect you with mental health support if needed.
This website does not provide medical advice.
The information, including but not limited to, text, graphics, images, and other material contained on this website is for informational purposes only. No material on this site is intended to be a substitute for professional medical advice, diagnosis, or treatment and/or medical treatment of a qualified physician or healthcare provider. EUFOREA is not a medical organisation and cannot provide specific medical advice to patients via the Internet and/or E-mail. All patients are encouraged to direct their specific questions to their personal physicians. EUFOREA presents this information to patients so that patients can understand and participate in their own medical care. EUFOREA strongly emphasises that the information contained on this website is not a substitute for thorough evaluation and treatment by a qualified healthcare provider.
© 2025 - EUFOREA - All rights reserved. All content on this portal, such as text, graphics, logos and images, is the property of EUFOREA. They may not be reproduced, copied, published, stored, modified or used in any form, online or offline, without prior written permission of EUFOREA.